|
Corresponding author: Stefka Ivanova ( ivanovastefka_pharm@yahoo.com ) Academic editor: Plamen Peikov
© 2022 Stefka Ivanova.
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC BY 4.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Citation:
Ivanova S (2022) Comparative assessment of clinical trials, indications, pharmacokinetic parameters and side effects of approved platinum drugs. Pharmacia 69(1): 1-7. https://doi.org/10.3897/pharmacia.69.e78813
|
Abstract
Platinum complexes are among the most commonly applied anticancer agents. The aim of current work is collection, analysing and comparative estimation of clinical trials and pharmacological indications of currently approved for application platinum detivatives: Cisplatin, Carboplatin, Oxaliplatin, Nedaplatin (Japan), Lobaplatin (China), Heptaplatin (North Korea), and Satraplatin. The other aim of the study includes the summarizing of the hystoric data for the stages of the developlement of these drugs, and the comparison of pharmacokimetic parameters, side effecs and the dose-liniting factors of the drugs. The observational study on pharmacokinetic parameters shows that protein binding decreases in order: 95% (Cisplatn); 90% (Oxaliplatin); 50% (Nedaplatin); low (Carboplatin). For every of Cisplatin, Carboplatin, Oxaliplatin have been reported more than 1000 clinical trials; for Lobaplatin, Nedaplatin, Satraplatin - about 10 trials. The differenses in dose-limiting effects are: neuro-, nephro-, ototoxicity (Cisplatin); neurotoxicity (Oxaliplatin); nephrotoxicity (Heptaplatin); myelosuppression: thrombocytopenia, neutropenia, leukopenia (Carboplatin, Nedaplatin, Satraplatin).
Keywords
application, Cisplatim derivatives, limiting factors
Introduction
Malignant tumors are the leading cause of lethality worldwide, and are a group of more than 100 different types of diseases, that are characterized by uncontrolled cell growth, local tissue invasion and distant metastases. The incidence of malignant tumors is enlarging, with the fastest increasing of lung, prostate, and colon cancers in men and breast carcinomas in women. Malignant tumors originate from different types of tissues: connective, epithelial, hematopoietic, lymphoid, nervous. Tumor cells are characterized by high mitotic and proliferative activity, have a shorter cell cycle duration, and a lower rate of cell death. The main difference between a normal and a tumor cell is the continuous tumor growth. Highly differentiated tumors have slower growth, metastasize relatively less frequently and later, and are less sensitive to cytostatics. Poorly differentiated cells proliferate rapidly, metastasize to distant organs, and are sensitive to cytostatics.
In carcinogenesis (oncogenesis, tumorigenesis) normal cells are transformed into cancer cells. This multistage process involves changes at the cellular and genetic levels, and involves initiation, promotion, malignant formation, progression, local tissue invasion and metastases. Initiation is characterized with the alteration, change, or mutation of genes. Genetic alterations are result from dysregulation of biochemical signaling pathways, associated with cellular proliferation, survival, and differentiation. The actively proliferating preneoplastic cells accumulate in the promotion stage. Progression is the final stage of neoplastic transformation, and is the phase between a premalignant lesion and the development of invasive cancer. Fast increase in the tumor size, genetic and phenotypic changes, and cell proliferation occur in progression phase. Metastasis is the spread of cancer cells through the bloodstream or the lymph system, from the primary site to other parts of the body (
The most significant risk factor for the development of cancer are genetic and environmental factors (
Genetic abnormalities include the following genes (
- cell cycle genes: p53 (brain and breast cancer); p16 (melanoma); Rb1 (retinoblastoma); VHL (renal cancer); WT1 (Wilms cancer)
- DNA repair genes: BRCA1, BRCA2 (breast cancer); MLH1, MSH2, MSH6, PMS1, PMS2 (colon cancer); XPA, XPB, XPC, XPD, XPF, XPG (skin cancer)
- signal transduction genes: MET (papillary renal cell carcinoma); NF1 (neurofibroma); RET (adrenal pheochromocytoma)
- genes responsible for tissue organization: APC (colon cancer); E-cadherin (gastric cancer); NF2 (neurinoma).
DNA damage can also be caused by substances, produced in the body. Macrophages and neutrophils in an inflamed colonic epithelium initiate colonic tumorigenesis (Anisimov VN et al. 2009), due to the DNA damage by reactive oxygen species. In high-fat diet, high levels of bile acids cause DNA damage, and contribute to colon cancer (
DNA damage can arise too from exposure to exogenous environmental carcinogenic agents:
- Physical factors
- ionized radiation: gene mutation or chromosome aberration in lung and thyroid cancer
- UV-light from solar radiation: DNA damage in melanoma (
Kanavy and Gerstenblith 2011 )
- Chemical factors
- benzo-pyrene: from tobacco smoke (
Kuper et al. 2002 ): lung cancer, due to mutation in the p53 gene, a tumor suppressor gene, which is considered to be one of the mechanisms of carcinogenesis (Saeki et al. 2000 ) - ethyl alcohol: esophageal cancer, due to p53 gene abnormalities (
Saeki et al. 2000 ) - cadmium: prostate cancer. (
Irigaray et al. 2007 ) -
Aspergillus flavus
metabolite aflatoxin: liver cancer (
Smela et al. 2002 ) - heterocyclic amines: overcooked meat and fish (de Verdier et al. 1991)
- Biological factors
-
Helicobacter pylori
infection: produces gastric cancer (
Handa et al. 2011 ) - Hepatitis B virus or Hepatitis C virus: liver cancer.
- Human T-lymphotrophic virus type 1: T cell lymphoma
- Human papilloma virus: esophagus cancer (
Siddiqui et al. 2015 ), chronic bacterial and parasitic infections (Samaras et al. 2010 ).
Cytotoxic chemotherapy has proven useful in a number of different cancer types including: lung, pancreatic and colorectal ca Concer (
Currently used in clinical practice: worldwide Cisplatin, Carboplatin, Oxaliplatin, Nedaplatin (registered in Japan), Lobaplatin (approved in China), Heptaplatin (South Korea), Satraplatin - for oral administration (Ndagi et al. 2020).
In the following tables are summarized produsers (Table
| Drug | Produsers |
|---|---|
| Cisplatin | Bristol-Myers, National Cancer Institute, Johnson Matthey and Engelhard Industries (USA) |
| Carboplatin | Bristol-Myers Squibb, Johnson Matthey, Cancer Research Institute, Marsden Royal Hospital, London |
| Oxaliplatin | Sanofi-Aventis, Roger Bellon Laboratories, Debiofharm Laboratories, Sanofi-Synthelabo Labotories |
| Nedaplatin | Shionogi Pharmaceutical (Osaka, Japan) |
| Heptaplatin | Sunkyong Industry (SK Chemicals, Kyungki-Do) |
| Lobaplatin | ASTA Medica (Germany), Zentaris AG, Hainan Tianwang (Chang’an) International Pharmaceutical |
| Satraplatin | Institute for Cancer Research in London and Johnson Matthey/AnorMed |
| Drug | Chemca name | Additional name |
|---|---|---|
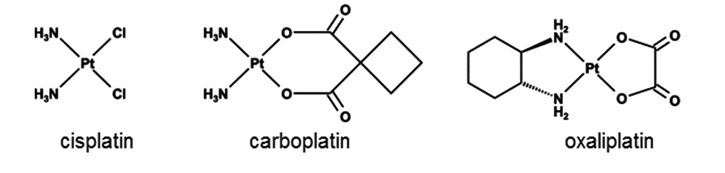
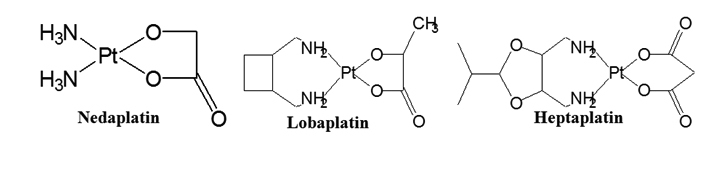
| Cisplatin | cisdiamminedichloroplatinum II | CDDP |
| Carboplatin | cis-diamine-(1,1-cyclobutanedicarboxylate) Pt II | Paraplatin, JM 8 |
| Oxaliplatin | 1R,2R-diaminocyclohexane oxalate Pt II | Eloxatin |
| Nedaplatin | cis-diamine-glycolate-O¹,O²) Pt II | 254-S |
| Lobaplatin | cis-(trans-1,2-diaminocyclobutane-lactato) Pt II | D-19466 |
| Heptaplatin | cis-malonato((4R,5R)-4,5-bis (aminomethyl)-2-isopropyl-1,3-dioxo-lane) Pt II | SKI2053R |
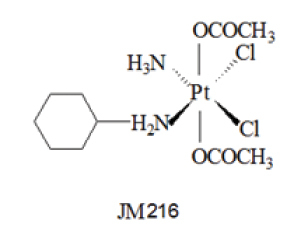
| Satraplatin | bis(acetato)amminedichlorocyclohexylamine Pt IV | JM 216 |
The development of the therapy is presented in Table
| Year | Cisplatin |
|---|---|
| 1845 | The earliest preparation of Cisplatin by the Italian chemist Michele Peyrone. |
| 1965 | Discovering of biological activity of Cisplatin by Barnet Rosenberg |
| 1966 | Confirmation of cis-geometry of Cisplatin by an X-ray method. |
| 1968 | The earliest pvoved activity of Cisplatin against model mice timors. |
| 1970 | Cisplatin enters clinical trial in non-small cell lung cancer. |
| 1971 | The earliest application of Cisplatin in patients. |
| 1975 | The beginning of Phase II clinical trials for Cisplatin. |
| 1978 | The approval of Cisplatin by the Food and Drug Administration. |
| 1978 | The authorisation of Platinol. |
| 1979 | The intraduction for Cisplatin in the United Kingdom. |
| 1979 | The approval for Platinex in Germany. |
| 1985 | Description of various cisplatin-induced adducts formed on DNA. |
| 1987 | The authorisation for Cisplatin in Austria. |
| 1991 | Role of elevated glutathione in inducing tumor resistance to Cisplatin. |
| 1996 | The generic Cisplatin Hospira receives marketing authorisation. |
| 1998 | The intraduction for Cisplatin as generic product of Teva Sante in France. |
| 1999 | Identification of the molecular defect that causes hypersensitivity of some testicular cancers to Cisplatin. |
| 2002 | Identification of the role of the CTR1 in transporting Cisplatin into cells. |
| Carboplatin | |
| 1982 | The earliest application of Carboplatin in patients. |
| 1988 | The approval of Carboplat in Germany. |
| 1989 | The authorisation of Carboplatin by FDA (ovarian cancer). |
| 1989 | The introduction from FDA of Paraplatin (Bristol-Myers Squibb) |
| 1990 | The approval of Carboplatin in the United Kingdom for ovarian carcinoma. |
| 1992 | The authorisation in France of Carboplatin, developed by Pfizer. |
| 1995 | The introduction of Carboplatin in Austria. |
| 2006 | FDA regulatory approval of Bevacizumab for the treatment of non-small cell lung cancer in combination with Carboplatin and Paclitaxel. |
| Year | Oxaliplatin ( |
|---|---|
| 1996 | Firstly approval for the second-line treatment of Oxaliplatin under the trade name Eloxatin (Sanofi Aventis). |
| 1998 | The authorisation of Eloxatin for advanced colorectal cancer. |
| 1999 | The introduction of Eloxatin iu major Europe states. |
| 1992 | First clinical study, demonstrating the effect of Oxaliplatin in combination with 5-Fluorouracil in patients with colorectal cancer. |
| 2002 | Oxaliplatin FDA regulatory approval for use in the treatment of colorectal cancer. |
| 2004 | Combination therapy: Oxaliplatin, 5-Fluorouracil and Leucovorin |
|
Nedaplatin ( |
|
| 1986 | Firstly prepared by Totani et al. in Japan ( |
| 1998 | The approval of Nedaplatin for clinical application in Japan. |
|
Lobaplatin ( |
|
| 1992 | The introduction of Lobaplatin into clinical trials. |
|
Picoplatin ( |
|
| 1997 | The earliest Picoplatin administration in patients with small cell lung cancer. |
|
Satraplatin ( |
|
| 1993 | Oral administration for the first time of Satraplatin to patients. |
| 2007 | Satraplatin FDA regulatory approval for the treatment of prostate cancer. |
Cisplatin as Peyrone’s chloride has been prepated by the Italian chemist Michele Peyrone For the generic Cisplatin Hospira, the approved indication spectrum is wider than that authorised by FDA (advanced or metastatic testicular, ovarian and bladder cancer), and includes: non-small and small cell lung carcinoma, squamous cell carcinoma of the head and neck, and cervical carcinoma, when combined with chemo- or radiotherapy. In Germany Platinex has been approved on for treatment of testicular, ovarian, and bladder cancer. The indication spectrum for Carboplat is for epithelial ovarian cancer, small cell lung carcinoma, squamous carcinoma of the head and neck, and metastatic cervical and ovarian cancer. In Austria Carboplatin indications includes: bladder cancer, squamous carcinoma of the head and neck, non-small cell lung cancer, and cervical carcinoma (
The chemical structures of approved platinum drugs are illustrated on Table
The most importamnt pharmacokinetic parameters for approved platinum drugs.
| Pharmacokinetic parameters | Cisplatin | Carboplatin ( |
Oxaliplatin | Nedaplatin |
|---|---|---|---|---|
| Bioavailability | 100% | 100% | 15% | good |
| Distribution volume | 11–12 l | 16 l | 440 l | 12 l |
| Protein binding | > 95% | low ( |
> 90% | 50% |
| Elimination half-life | 30–100 h | 2.6–5.9 h | 10–25 min | - |
| Excretion | renal | renal | renal | renal |
Cisplatin is binding to plasma proteins: gammaglobulin, albumin, transferrin, and 90% of the plasma platinum is protein-bound 2 h after 3 h infusion. Cisplatin concentrations are highest in liver, kidney, prostate; lower in muscle, pancreas, spleen, bladder, and lowest in cerebrum, cerebellum, lung, heart, adrenal. In tissues platinum is present 6 months after the last administration. The complexes between albumin and Cisplatin do not dissociate to a significant extent, and are eliminated slowly with a minimum half-life of 5 days or more.
The distribution half-life of Carboplatin is 1.1–2 h. Predominantly the drug is elimi-nated in the urine as the unchanged parent compound: 65% within 12 h, 71% within 24 h; 5% from 24 h to 96 h, withouth biliary elimination. The total body clearance after a 30 min. intravenous infusion of 500 mg/m2 is 4.4 l/h (
The indications for the approved platinum drugs are presented in Table
| Drug | Indications |
|---|---|
| Cisplatin | ovarian ( |
| Carboplatin | ovarian, cervical, testicular, brain, bladder, breast, head, neck and lung cancers, retinoblastoma, neuroblastoma, nephroblastoma ( |
| Oxaliplatin | ovarian, breast, head and neck cancer, non-Hodgkin’s lymphoma, malignant melanoma, glioblastoma, NSCLC, neuroendocrine tumors ( |
| Nedaplatin | head, neck, esophagus, small cell lung, non-small cell lung cancer, ovarian, testicular, prostate, cervical cancer ( |
| Heptaplatin | gastric (Hong et al. 1996), small cell lung cancer ( |
| Lobaplatin | chronic myelocytic leukemia, small-cell lung, breast, gastric cancer, esophageal squamous cell and hypopharyngeal carcinoma, osteosarcoma ( |
| Satraplatin | lung, breast, cervical, prostate and ovarian cancer ( |
The data for the clinical trials are shown on Table
| Cisplatin (https://go.drugbank.com/drugs/DB00515) | |
|---|---|
| Cancers | Brain; Head and Neck; Hypopharyngeal; Laryngeal; Oropharyngeal; Small Cell Lung; Non-Small Cell Lung; Breast; Peritoneal Cavity; Liver; Bladder; Cervical; Endometrial; Extragonadal; Prostate |
| Adenocarcinomas | Lung; Esophageal; Gastroesophageal; Stomach; Pancreatic; Cervical; Endometrial |
| Carcinomas | Head and Neck; Salivary Gland; Tongue; Esophageal squamous cell; Hypopharyngeal; Laryngeal; Nasopharyngeal; Oropharyngeal; Non-Small Cell Lung; Lung Squamous; Squamous Cell; Bladder; Biliary Tract; Urothelial; Cervical; Ovarian; Adrenocortical; Intrahepatic Cholangiocarcinoma |
| Neoplasms | Brain; Head and Neck; Esophageal; Nasopharyngeal; Gastric; Pancreas; Testicular |
| Lymphoms | Nasal; Peripheral T Cell; Hodgkin |
| Blastomas | Hepatoblastoma; Medulloblastoma |
| Other | Melanoma; Mesothelioma; Nasopharyngeal Lymphoepithelioma; Sarcoma |
| Carboplatin (https://go.drugbank.com/drugs/DB00958) | |
| Cancers | Brain; Neuroendocrine; Head and Neck; Small Cell Lung; Non-Small Cell Lung; Breast; Gastroesophageal; Peritoneal; Cervical; Ovarian; Endometrial; Extragonadal; Embryonal |
| Carcinomas | Neuroendocrine; Esophageal; Non-Small Cell Lung; Lung Squamous; Squamous Cell; Colorectal, Urothelial; Hepatocellular; Cervical |
| Neoplasms | Esophageal; Lung; Breast; Abdominal wall; Cervical; Ovarian |
| Lymphoms | Non-Hodgkin‘s |
| Blastomas | Neuroblastoma; Medulloblastoma; Retinoblastoma |
| Other | Lung adenocarcinoma; Mesothelioma |
| Lobaplatin (https://go.drugbank.com/drugs/DB13049) | |
| Cancer | Small Cell Lung; Breast |
| Carcinoma | Hed and neck; Esophagea; Nasopharyngeal; Hepatocellular |
| Neoplasm | Stomach |
| Other | Osteosarcoma |
| Oxaliplatin (https://go.drugbank.com/drugs/DB00526) | |
|---|---|
| Adeno-carcinoma | Esophageal; Gastroesophageal; Gastric; Pancreas; Colorectal; Bowel; Cervix |
| Cancers | Brain; Breast; Esophageal; Gastric; Gastroesophageal; Pancreatic; Peritoneal; Colon; Colorectal; Biliary Tract; Liver; Cervical; Ovarian; Prostate |
| Carcinomas | Neuroendocrine; Non-Small Cell Lung; Esophageal; Gastroesophageal; Pancreatic; Peritoneal; Colorectal; Rectal; Hepatocellular; Cervical; Ovarian |
| Neoplasms | Esophageal; Nasopharyngeal; Breast; Gastrointestinal; Pancreatic; Colorectal Hepatic; Biliary Tract |
| Lymphoms | Non-Hodgkin’s; Nasal; NK-T-Cell; B-Cell |
| Blastomas | Hepatoblastoma |
| Nedaplatin (https://go.drugbank.com/drugs/DB13145) | |
| Cancers | Small Cell Lung; Gastric; Ovarian; Cervical |
| Carcinoma | Head and Neck; Esophageal; Nasopharyngeal; Non-Small Cell Lung |
| Neoplasms | Esophageal |
| Satraplatin (https://go.drugbank.com/drugs/DB04996S) | |
| Cancers | Breast Lung Prostate |
| Carcinoma | Non-Small Cell Lung |
| Neoplasms | Brain |
Neurotoxicity is the most important adverse effect of Cisplatin chemotherapy in 47% of patients Symptoms include numbness, tingling, paraesthesia in the limbs, difficulty walking, decreased sensation of tendon reflexes Neuropathy is long-term with significant worsening of symptoms during the first 4 months, which may continue 52 months after stopping treatment. Higher concentrations in peripheral nervous system tissues (peripheral nerves and dorsal root ganglia), compared to central nervous system tissues (brain, spinal cord) correlate with clinical symptoms of peripheral neuropathy.
Toxicity of platinum compounds is presented on Table
Toxicity of approved platinum drugs (
| Drug | Side-effects | Dose-limiting side effects |
| Cisplatin | nausea, vomiting, electrolyte disturbance: hypomagnesaemia, hypokalaemia and hypocalcaemia. hemolytic anemia ( |
neurotoxicity, hearing disorder, paraesthesia, sensory ataxia ( |
| Carboplatin | neuropathy, nephro-, oto- and gastrointestinal toxicity ( |
myelosuppression: thrombocytopenia, neutropenia, leukonia ( |
| Oxaliplatin | neutropenia, ototoxicity, fatigue, nausea, vomiting, diarrhea ( |
neurotoxicity ( |
| Nedaplatin | nephro-, neuro-, gastrointestinal toxicity ( |
myelosuppression: thrombocytopenia neutropenia, leucopenia, anemia |
| Heptaplatin | leukopenia, thrombocytopenia, neurohepato-, embryotoxicity ( |
nephrotoxicity ( |
| Satraplatin | granulocytopenia, anemia, diarrhea, constipation, nausea, vomiting ( |
thrombocytopenia, leucopenia, neutropenia |
Recent developments in antitumor coordination compounds (
Concluson
More than 1000 clinical trials have been reported for every of the following anticancer agents: Cisplatin, Carboplatin, Oxaliplatin. The more investigations have been applied for Cisplatin. In comparison, for Lobaplatin, Nedaplatin, and Satraplatin have been reported very few clinical trials – about 10 for every drug. The following differenses in dose-limiting effects have been reported: neuro-, nephro-, and ototoxicity (Cisplatn); neurotoxicity (Oxaliplatin); nephtotoxicity (Heptaplatin); myelosuppression: thrombocytopenia, neutropenia and leukonia (Carboplatin, Nedaplatin, Satraplatin).
Conflict of interests
There are no conflict of interests.
Referensess
- Ahn JH, Kang YK, Kim TW, Bahng H, Chang HM, Kang WC, Kim WK, Lee JS, Park JS (2002) Nephrotoxicity of Heptaplatin: a randomized comparison with Cisplatin in advanced gastric cancer. Cancer Chemotherapy and Pharmacology 50(2): 104–110. https://doi.org/10.1007/s00280-002-0483-x
- Anisimov VN, Sikora E, Pawelec G (2009) Relationships between cancer and aging: a multilevel approach. Biogerontol 10(4): 323–338. https://doi.org/10.1007/s10522-008-9209-8
- Argyriou AA, Polychronopoulos P, Iconomou G, Chroni E, Kalofonos HP (2008) A review on Oxaliplatin-induced peripheral nerve damage. Cancer Treatment Reviews 34(4): 368–377. https://doi.org/10.1016/j.ctrv.2008.01.003
- Avan A, Postma TJ, Ceresa C, Avan А, Cavaletti G, Giovannetti E, Peters GJ (2015) Platinum-induced neurotoxicity and preventive strategies: past, present, and future. The Oncologist 20(4): 411–432. https://doi.org/10.1634/theoncologist.2014-0044
- Bernstein C, Holubec H, Bhattacharyya AK, Nguyen H, Payne CM, Zaitlin B (2011) Bernstein H. Carcinogenicity of deoxycholate, a secondary bile acid. Archives of Toxicology 85(8): 863–871. https://doi.org/10.1007/s00204-011-0648-7
- Bhargava A, Vaishampayan UN (2009) Satraplatin: leading the new generation of oral platinum agents. Expert Opinion on Investigational Drugs 18(11): 1787–1797. https://doi.org/10.1517/13543780903362437
- Cassidy J, Misset JL (2002) Oxaliplatin-related side effects: characteristics and management. Seminars in Oncology 29(5)(Suppl 15): 11–20. https://doi.org/10.1053/sonc.2002.35524
- Chay WY, Chew L, Yeoh TT, Tan MH (2010) An association between transient hypokalemia and severe acute Oxaliplatin-related toxicity predominantly in women. Acta Oncologica 49(4): 515–517. https://doi.org/10.3109/02841860903464015
- Chung MK, Kim JC, Roh JK (1988) Embryotoxic effects of SKI 2053R, a new potential anticancer agent, in rats. Reproductive Toxicology 12(3): 375–381. https://doi.org/10.1016/s0890-6238(98)00016-1
- Corrie GP (2008) Cytotoxic chemotherapy: clinical aspects. Medicine 36(1): 24–28. https://doi.org/10.1016/j.mpmed.2007.10.012
- Dasari S, Tchounwou PB (2014) Cisplatin in cancer therapy: molecular mechanisms of action. European Journal of Pharmacology 740(1): 364–378. https://doi.org/10.1016/j.ejphar.2014.07.025
- de Sousa GF, Wlodarczyk RS, Montei G (2014) Carboplatin: molecular mechanisms of action associated with chemoresistance Brazilian Journal of Pharmaceutical Sciences 50(4): 693–700. https://doi.org/10.1590/S1984-82502014000400004
- de Verdier MG, de Sousa GF, Wlodarczyk RS, Montei G (2014) Carboplatin: molecular mechanisms of action associated with chemoresistance Brazilian Journal of Pharmaceutical Sciences 50(4): 693–700. https://doi.org/10.1590/S1984-82502014000400004
- Decatris MP, Sundar S, O’Byrne KJ (2004) Platinum-based chemotherapy in metastatic breast cancer: current status. Cancer Treatment Reviews 30(1): 53–81. https://doi.org/10.1016/S0305-7372(03)00139-7
- Degardin M, Armand JP, Chevallier B, Cappelaere P, Lentz MA, David M, Roché H (1995) A clinical screening cooperative group phase II evaluation of Lobaplatin (ASTA D-19466) in advanced head and neck cancer. Investigational New Drugs 13(3): 253–255. https://doi.org/10.1007/BF00873809
- Desoize B, Madoulet C (2002) Particular aspects of platinum compounds used at present in cancer treatment. Critical Reviews in Oncology/Hematology 42(3): 317–325. https://doi.org/10.1016/s1040-8428(01)00219-0
- Dhar S, Kolishetti N, Lippard SJ, Farokhzad OC (2011) Targeted delivery of a Cisplatin prodrug for safer and more effective prostate cancer therapy in vivo. Proceedings of the National Academy of Sciences of the United States of America 108(5): 1850–1855. https://doi.org/10.1073/pnas.1011379108
- Doneva N, Boseva N, Gencheva G, Tsekova D, Momekov G (2014) Oncopharmacological evaluation of cytotoxic platinum, palladium and gold metal complexes with porphyrin ligands, 115(1): 313–313.
- Gebremedhn EG, Shortland PJ, Mahns DA (2018) The incidence of acute Oxaliplatin-induced neuropathy and its impact on treatment in the first cycle: a systematic review. BMC Cancer 18(1): 410–410. https://doi.org/10.1186/s12885-018-4185-0
- Gencheva G, Tsekova D, Gochev G, Momekov G, Tyuliev G, Skumryev V, Karaivanova M, Bontchev PR (2007) Synthesis, structural characterization and cytotoxic activity of novel paramagnetic platinum hematoporphyrin IX complexes – potent antitumour agents, Metal-Based Drugs 2007(1): 1–13. [67376] https://doi.org/10.1155/007/67376
- Gienema JA, de Vries EG, Sleijfer DT, Willemse PH, Guchelaar HJ, Uges DR, Aulenbacher P, Voegeli R, Mulder NH (1993) A phase I study of 1,2-diamminomethylcyclobutane- platinum (II)-lactate (D-19466; Lobaplatin) administered daily for 5 days. British Journal of Cancer 67(2): 396–401. https://doi.org/10.1038/bjc.1993.73
- Hagman U, Peters RK, Steineck G, Overvik E (1991) Meat, cooking methods and colorectal cancer: a case-referent study in Stockholm. International Journal of Cancer 49(4): 520–525. https://doi.org/10.1002/ijc.2910490408
- Handa O, Naito Y, Yoshikawa T (2011) Redox biology and gastric carcinogenesis: the role of Helicobacter pylori. Redox Report 16(1): 1–7. https://doi.org/10.1179/174329211X12968219310756
- Hartmann JT, Lipp HP (2003) Toxicity of platinum compounds. Expert Opinion on Pharmacotherapy 4(6): 889–901. https://doi.org/10.1517/14656566.4.6.889
- Hong WS, Kim HT, Kim KH, Kim DK (1995) In vitro antitumor activity of a new platinum complex, cismalonato ((4R,5R)-4,5-bis(aminomethyl)-2-isopropyl-1,3-dioxolane) platinum (II) (SKI 2053R), against human lung and stomach cancer cell lines. Anticancer Res 15(1): 51–54. [PMID: 773364022]
- Ishibashi T, Yano Y, Oguma T (2003) Population pharmacokinetics of platinum after Nedaplatin administration and model validation in adult patients. British Journal of Clinical Pharmacology 56(2): 205–213. https://doi.org/10.1046/j.1365-2125.2003.01871.x
- Irigaray P, Newby JA, Clapp R, Hardell L, Howard V, Montagnier L, Epstein S, Belpomme D (2007) Lifestyle-related factors and environmental agents causing cancer: an overview. Biomedicine & Pharmacotherapy 61(10): 640–658. https://doi.org/10.1016/j.biopha.2007.10.006
- Kalayda GSG (2020) History of platinum-based drugs from a regulatory perspective. Thesis for Master of Drug Regulatory Affairs, Bonn.
- Kanavy HE, Gerstenblith MR (2011) Ultraviolet radiation and melanoma. Seminars in Cutaneous Medicine and Surgery 30(4): 222–228. https://doi.org/10.1016/j.sder.2011.08.003
- Koizumi W, Narahara H, Hara T, Takagane A, Akiya T, Takagi M, Miyashita K, Nishizaki T, Kobayashi O, Takiyama W, Toh Y, Nagaie T, Takagi S, Yamamura Y, Yanaoka K, Orita H, Takeuchi M (2008) S-1 plus Cisplatin versus S-1 alone for first-line treatment of advanced gastric cancer (SPIRITS trial): a phase III trial. The Lancet Oncology 9(3): 215–221. https://doi.org/10.1016/S1470-2045(08)70035-4
- Koshiyama M, Kinezaki M, Uchida T, Sumitomo M (2005) Chemosensitivity testing of a novel platinum analog, Nedaplatin (254-S) in human gynecological carcinomas: a comparison with cisplatin. Anticancer Research 25(6C): 4499–4502. [PMID: 16334133]
- Kuper H, Boffetta P, Adami HO (2002) Tobacco use and cancer causation: association by tumour type. Journal of Internal Medicine 252(3): 206–224. https://doi.org/10.1046/j.1365-2796.2002.01022.x
- Levi F, Metzger G, Massari C, Milano G. (2000)Oxaliplatin: pharmacokinetics and chronopharmacological aspects. Clinical Pharmacokinetics , 38(1): 1–21. https://doi.org/10.2165/00003088-200038010-00001
- Markman M (2003) Toxicities of the platinum antineoplastic agents. Expert Opinion on Drug Safety 2(6): 597–607. https://doi.org/10.1517/14740338.2.6.597
- Meng F, Sun G, Zhong M, Yu Y, Brewer MA (2013) Anticancer efficacy of Cisplatin and Trichostatin A or 5-aza-20-deoxycytidine on ovarian cancer. British Journal of Cancer. 108(3): 579–586. https://doi.org/10.1038/bjc.2013.10
- Miller RP, Tadagavadi RK, Ramesh G, Reeves WB (2010) Mechanisms of Cisplatin nephrotoxicity. Toxins (Basel) 2(11): 2490–2518. https://doi.org/10.3390/toxins2112490
- Minami D, Takigawa N, Takeda H, Takata M, Ochi N, Ichihara E, Hisamoto A, Hotta K, Tanimoto M, Kiura K (2013) Synergistic effect of Olaparib with combination of Cisplatin on PTEN-deficient lung cancer cells. Molecular Cancer Research 11(2): 140–148. https://doi.org/10.1158/1541-7786.MCR-12-0401
- Momekov G, Momekova D (2006) Recent developments in antitumor platinum coordination compounds. Expert Opinion on Therapeutic Patents 16(90): 1383–1403. https://doi.org/10.1517/13543776.16.10.1383
- Momekov G, Bakalova A, Karaivanova M (2005) Novel approaches towards development of non-classical platinum-based antineoplastic agents: design of platinum complexes characterized by an alternative DNA-binding pattern and/or tumor-targeted cytotoxicity. Current Medicinal Chemistry 12(19): 2177–2191. https://doi.org/10.2174/0929867054864877
- Momekov G, Ugrinova I, Pasheva E, Tsekova D, Gencheva G (2018) Cellular pharmacology of palladium (III) hematoporphyrin IX complexes: solution stability, antineoplastic and apoptogenic activity, DNA binding, and processing of DNA-adducts. International Journal of Molecular Sciences 19(8): 1–21. [2451] https://doi.org/10.3390/ijms19082451
- Momekov G, Ferdinandov D, Konstantinov S, Arpadjan S, Tsekova D, Gencheva G, Bontchev PR, Karaivanova M (2008) In vitro evaluation of a stable monomeric gold (II) complex with hematoporphyrin IX: cytotoxicity against tumor kidney cells, cellular accumulation and induction of apoptosis. Bioinorganic Chemistry and Applications 2008(1): 1–8. [367471] https://doi.org/10.1155/2008/367471
- Momekov G, Karaivanova M, Ugrinova I, Pasheva E, Gencheva G, Tsekova D, Arpadjan S, Bontchev P (2010) In vitro pharmacological study of monomeric platinum (III) hematoporphyrin IX complexes. Investigational New Drugs 29(5): 742–751. https://doi.org/10.1007/s10637-010-9412-8
- Monneret C (2011) Platinum anticancer drugs. From serendipity to rational design. Annales Pharmaceutiques Françaises 69(6): 286–295. https://doi.org/10.1016/j.pharma.2011.10.001
- Ndagi U, Mhlongo N, Soliman ME (2017) Metal complexes in cancer therapy – an update from drug design perspective. Drug Design, Development and Therapy 11(1): 599–616. https://doi.org/10.2147/DDDT.S119488
- Oguri S, Sakakibara T, Mase H, Shimizu T, Ishikawa K, Kimura K, Smyth RD (1988) Clinical pharmacokinetics of Carboplatin. Journal of Clinical Pharmacology 28(3): 208–215. https://doi.org/10.1002/j.1552–4604.1988.tb03134.x
- Oun R, Moussa YE, Wheate NJ (2018) The side effects of platinum-based chemotherapy drugs: a review for chemists. Dalton Transactions journal 47(19): 6645–6653. https://doi.org/10.1039/c8dt00838h
- Pabla N, Dong Z (2008) Cisplatin nephrotoxicity: mechanisms and renoprotective strategies. Kidney International 73(9): 994–1007. https://doi.org/10.1038/sj.ki.5002786
- Previati M, Lanzoni I, Corbacella E, Magosso S, Guaran V, Martini A (2006) Cisplatin-induced apoptosis in human promyelocytic cells. International Journal of Molecular Medicine 18(3): 511–516. https://doi.org/10.3892/ijmm.18.3.511
- Reece PA, Bishop JF, Olver IN, Stafford I, Hillcoat BL, Morstyn G (1987) Pharmacokinetics of unchanged Carboplatin (CBDCA) in patients with small cell lung carcinoma. Cancer Chemotherapy and Pharmacology 19(4): 326–330. https://doi.org/10.1007/BF00261482
- Saeki H, SugiIchi K (2001) Carcinogenic risk factors. JMAJ 44(6): 245–249.
- Saeki H, Ohno S, Araki K, Egashira A, Kawaguchi H, Ikeda Y, Morita M, Kitamura K, Sugimachi K (2000) Alcohol consumption and cigarette smoking in relation to high frequency of p53 protein accumulation in oesophageal sequamous cell carcinoma in the Japanese. British Journal of Cancer 82(11): 1892–1894. https://doi.org/10.1054/bjoc.1999.1212
- Samaras V, Rafailidis PI, Mourtzoukou EG, Peppas G, Falagas ME (2010) Chronic bacterial and parasitic infections and cancer: a review. Journal of Infection in Developing Countries 4(5): 267–281. https://doi.org/10.3855/jidc.819
- Sasaki Y, Tamura T, Eguchi K, Shinkai T, Fujiwara Y, Fukuda M, Ohe Y, Bungo M, Horichi N, Niimi S, Koichi Minato K, Nakagawa K (1989) Pharmacokinetics of (glycolate-0,0’)-diammine platinum (II), a new platinum derivative, in comparison with Cisplatin and Carboplatin. Cancer Chemotherapy and Pharmacology 23(4): 243–246. https://doi.org/10.1007/BF00451649
- Shaili E (2014) Platinum anticancer drugs and photochemotherapeutic agents: recent advances and future developments. Science Progress 97(1): 20–40. https://doi.org/10.3184/003685014X13904811808460
- Shimada M, Itamochi H, Kigawa J (2013) Nedaplatin: a cisplatin derivative in cancer chemotherapy. Cancer Management and Research 5(1): 67–76. https://doi.org/10.2147/CMAR.S35785
- Siddiqui IA, Sanna V, Ahmad N, Sechi M, Mukhtar H (2015) Resveratrol nanoformulation for cancer prevention and therapy. Annals of the New York Academy of Sciences 1348(1): 20–31. https://doi.org/10.1111/nyas.12811
- Smela ME, Hamm ML, Henderson PT, Harris CM, Harris TM, Essigmann JM (2002) The aflatoxin B(1) formamidopyrimidine adduct plays a major role in causing the types of mutations observed in human hepatocellular carcinoma. Proceedings of the National Academy of Sciences of the United States of America 99(10): 6655–6660. https://doi.org/10.1073/pnas.102167699
- Sooriyaarachchi M, Narendran A, Gailer J (2011) Comparative hydrolysis and plasma protein binding of Cisplatin and Carboplatin in human plasma in vitro. Metallomics 3(1): 49–55. https://doi.org/10.1039/c0mt00058b
- Spada F, Antonuzzo L, Marconcini R, Radice D, Antonuzzo A, Ricci S, Di Costanzo , Fontana A, Gelsomino F, Luppi G, Nobili E, Galdy S, Cella CA, Sonzogni A, Pisa E, Barberis M, Fazio N (2016) Oxaliplatin-based chemotherapy in advanced neuroendocrine tumors: clinical outcomes and preliminary correlation with biological factors. Neuroendocrinol 103(6): 806–814. https://doi.org/10.1159/000444087
- Totani T, Aono K, Komura M, Adachi Y (1986) Synthesis of (glycolato-O,O’) diammineplatinum (II) and it’s related complexes. Chemistry Letters 15(3): 429–432. https://doi.org/10.1246/cl.1986.429
- Waissbluth S, Daniel SJ (2013) Cisplatin-induced ototoxicity: transporters playing a role in Cisplatin toxicity. Hearing Research 299(1): 37–45. https://doi.org/10.1016/j.heares.2013.02.002
- Wheate NJ, Walker S, Craig GE, Oun R (2010) The status of platinum anticancer drugs in the clinic and in clinical trials. Dalton Trans 39(35): 8113–8127. https://doi.org/10.1039/c0dt00292e
- Wu X, Tang P, Li S, Wang S, Liang Y, Zhong L, Ren L, Zhang T, Zhang Y (2018) A randomized and open-label phase II trial reports the efficacy of neoadjuvant Lobaplatin in breast cancer. Nature Communications 9(1): 1–8. [832] https://doi.org/10.1038/s41467-018-03210-2
- Yao X, Panichpisal K, Kurtzman N, Nugent K (2007) Cisplatin nephrotoxicity: a review. The American Journal of the Medical Sciences 334(2): 115–124. https://doi.org/10.1097/MAJ.0b013e31812dfe1e
- Zang DY, Lee KH, Lee JS, Lee JH, Kim WK, Kim SH, Kim WD, Kim DS, Kim JH, Kim BS, Cho YB, Kim DK, Kim KH (1999) Phase II trial of a novel platinum analog, SKI 2053R, in patients with previously untreated extensive-stage small-cell lung cancer. American Journal of Clinical Oncology 22(5): 495–498. https://doi.org/10.1097/00000421-199910000-00015